- History of complicated withdrawal (delirium tremens, seizures, ICU admission)
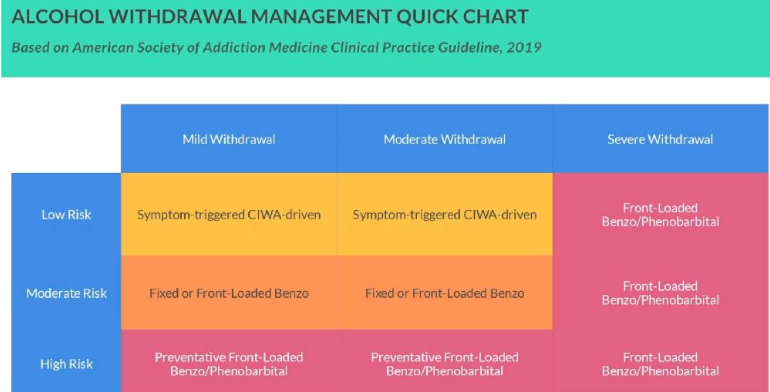
- At risk for severe or complicated alcohol withdrawal
- Actively withdrawing despite high blood alcohol level
- Actively withdrawing means CIWA>7
- Discontinue prophylaxis once 6 CIWA scores concurrently <8
- very concerning if high BAL and CIWA > 7
- Delirium or encephalopathy
- Benzodiazepine non-response or benzodiazepine resistance
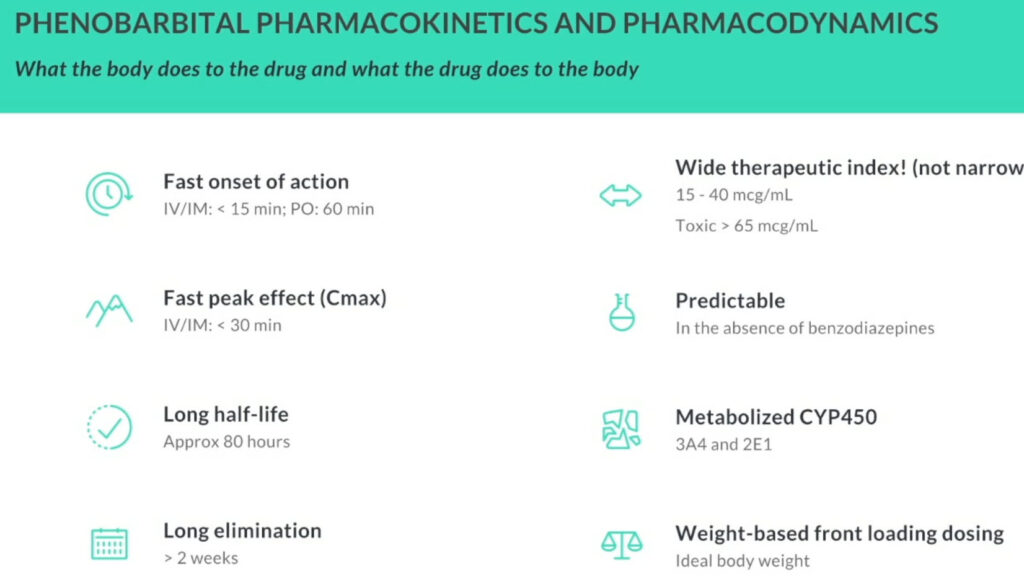
- Phenobarbital tends to be less deliriogenic
- Excessive drinking results in the down-regulation of inhibitory GABA receptors
- Down-regulation of GABA receptors leads to up-regulation of excitatory receptors to maintain homeostasis
- Homeostasis regained until take alcohol away→ dysregulation of inhibitory + excitatory neurotransmitters
- Super excitation of glutamate receptors created→ withdrawal symptoms


- Phenobarbital is very predictable.
- Using 10mg/kg IDW dose almost impossible to cause toxic level in absence of benzodiazeipines.
- Determine risk of severe or complicated withdrawal syndrome→ PAWS scale
- Determine risk of complications
- Sedation→ > 65 yo, hepatic dysfunction, narcotics, head injury, recent sedatives
- Respiratory compromise→ pneumonia, rib fractures, chest tube, contusion, C-collar/ brace
- chronic issues not a concern (COPD, Asthma, OSA)
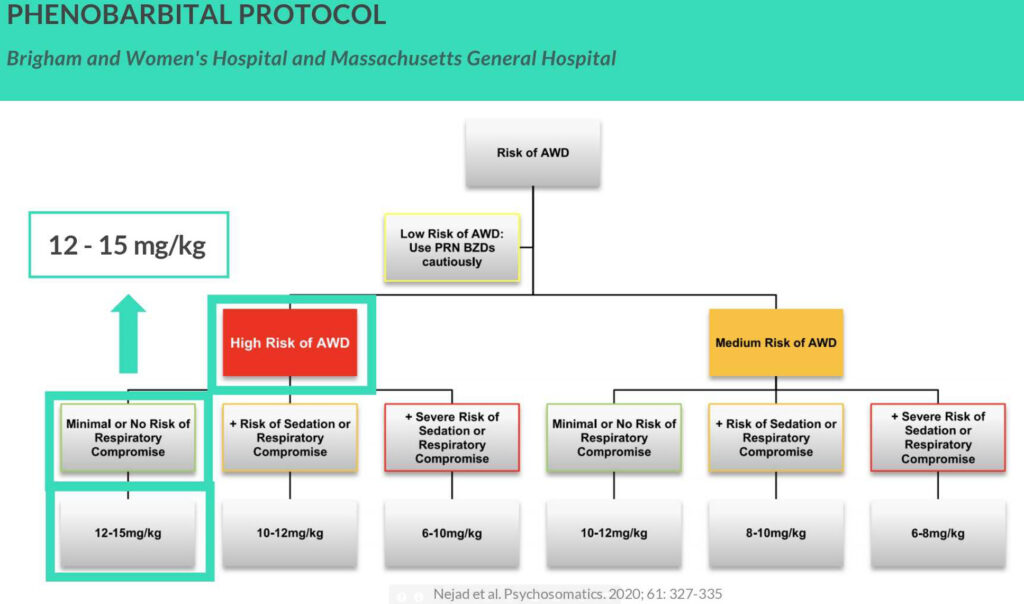
- Algorithm will guide you to loading dose
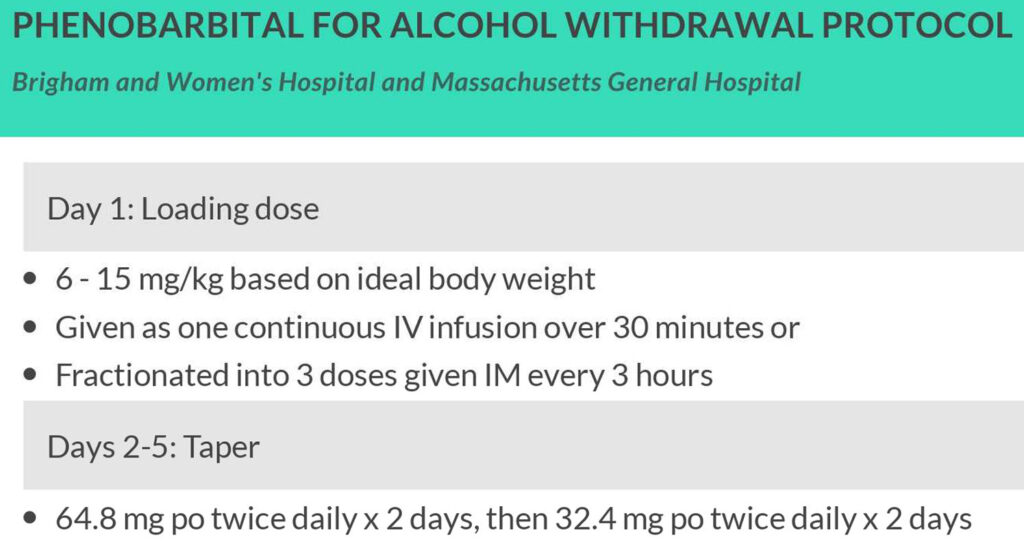
- Day 1: Loading Dose
- 6-15 mg/kg IDW
- one continuous IV infusion over 30 mins (may have to do in ED/ICU)
- or Fractionated into 3 doses given IM every 3 hrs
- Day 2-15: Taper
- 64.8 mg PO twice daily x 2 days, then 32.4 mg PO twice daily x 2 days
- does not have to be completed, if doing well can be stopped early
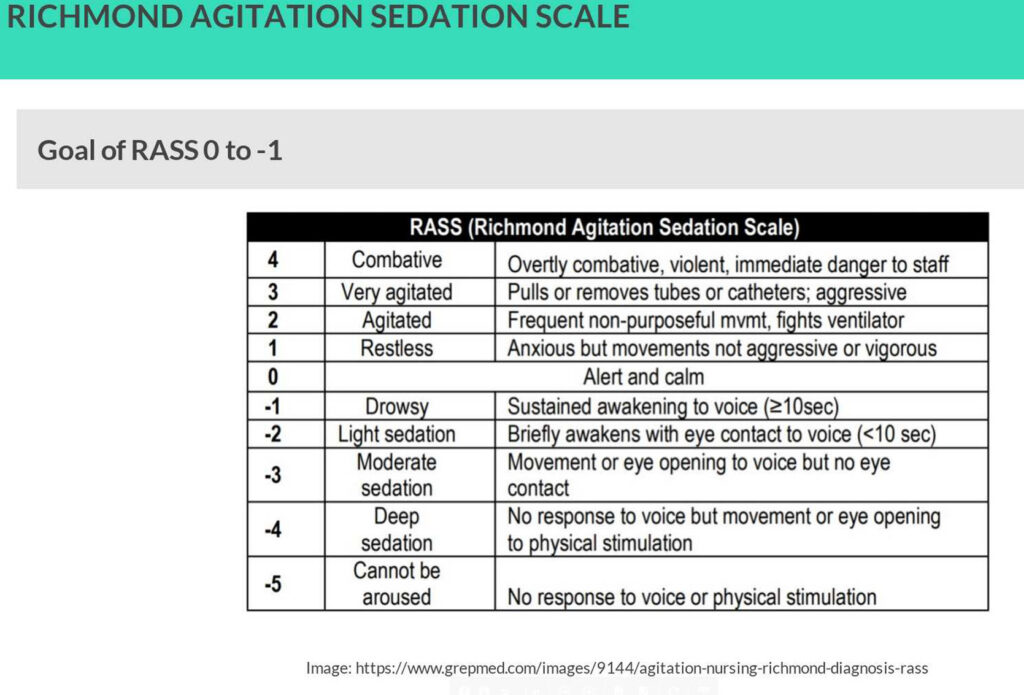
- Give phenobarbital 65-130mgs IV/IM/PO every 1 hour as needed to achieve RASS goal of 0 to -1
- not at risk of dose stacking due to fast onset
- Max cumulative dose 20-30mg/kg- rare to get there, usually 10-15 mg/kg enough
- use caution with <10mg/kg- few pts truly at high risk for mod-severe withdrawal that will get by on this dose
- Consider adding non-GABA-ergic medication→ haloperidol
- avoid benzodiazepines after this large loading dose
- many programs use phenobarb+ benzos but only with smaller phenobarbital loading doses
- once go down this road with phenobarbital, you will not be able to turn back
- <72 hours
- alcohol withdrawal seizures: 24-48 hrs
- delirium tremens: 48-90 hrs
- consider increasing dose of benzodiazepine, switching to IV or switching to phenobarbital
- if guess wrong and decrease dose to soon, could put pt at higher risk of these complications to develop
- Goal RASS -1
- >72 hours
- consider benzodiazepine-induced delirium
- reduce dose of benzodiazepine & add antipsychotic (risperidone, quetiapine, haloperidol)
- look for other non-alcohol related causes
- consider using gabapentin, valproic acid & clonidine if not 1st-line